Absolute cardiovascular risk in clinical practice
Cardiovascular disease (CVD) continues to be a major cause of disease and death in Australia. This is despite being preventable in many cases. Current Australian and international guidelines encourage absolute CVD risk assessment to guide treatment decisions in primary prevention.
Key Points
- Use absolute risk to calculate CVD risk in the next 5 years for adults aged from 45 years (or 35 years for Aboriginal and Torres Strait Islanders).
- Not all adults will need absolute risk calculated as they may already be at clinically determined high risk of CVD.
- Clinical judgement remains a key requirement when assessing absolute risk, especially for specific populations.
- Aboriginal and Torres Strait Islanders people >74 years are clinically determined high risk.
Absolute CVD risk assessment describes the likelihood (expressed as a percentage) that an individual will experience a CV event within a given time period (usually 5 or 10 years).1, 2
Australian guidelines calculate absolute risk using an equation model based on data from the long-running Framingham Study.1 This risk equation accounts for several contributors to cardiovascular disease in an individual, has been validated in non-Indigenous Australian adults and categorises absolute risk as low (<10% likelihood of CVD event over 5 years), moderate (10–15%) or high (> 15%).1
Using absolute risk within clinical practice
In adults, assess absolute cardiovascular risk from 45 years (or 35 years for Aboriginal and Torres Strait Islanders) according to the algorithm below.1
Be aware that there are parameters defining appropriate use of this assessment tool within clinical practice, especially for use in populations not represented in the Framingham study (e.g. older people > 74 years, Aboriginal and Torres Islander peoples).
Absolute risk calculator is only applicable for primary prevention
Absolute risk calculators are useful for measuring risk in asymptomatic patients without CVD (ie primary prevention).1 The calculators have not been validated for use in people with established CVD (ie, coronary heart disease, stroke, peripheral arterial disease, some types of kidney disease) who should be treated as high risk and managed accordingly
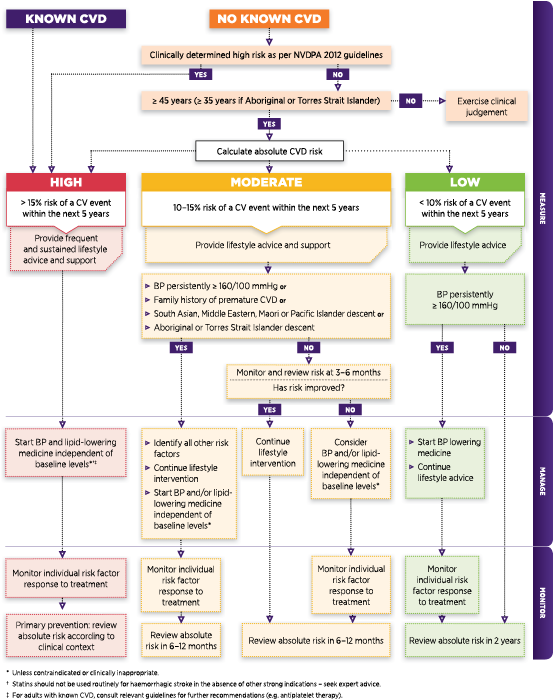
Cardiovascular disease (CVD) risk assessment and management algorithm1
Adapted with permission from NVDPA
Some patients without CVD are automatically determined as high risk
Not all individuals need a formal absolute CVD risk calculation (regardless of their age) because they are already clinically determined to be at high risk of a cardiovascular event.1 This group includes those with:
- diabetes and age 60 years
- diabetes with microalbuminuria (20 micrograms/min or urinary albumin:creatinine ratio;2.5 mg/mmol for males, 3.5 mg/mmol for females)
- moderate or severe chronic kidney disease (eGFR 45 mL/min/1.73 m2)
- previous diagnosis of familial hypercholesterolaemia
- systolic BP ≥180 mm Hg; or diastolic BP ≥ 110 mm Hg
- serum total cholesterol 7.5 mmol/L
- Aboriginal and Torres Strait Islander adults aged over 74 years
Absolute risk equations underestimate risk in certain groups
Some patients carry risk factors that can impact on CVD but have not been included within the current absolute risk equation. Other patients belong to populations that are outside those upon which the risk models are based.3-5
As a result, using absolute risk can be somewhat limited and may represent only part of the risk estimate (eg, underestimate risk). In many of these patients absolute risk assessments can be taken as a good estimate of the minimum risk and interpretation of risk with subsequent treatment decisions needing to be guided by clinical judgement.1 For example, in overweight or obese patients not at calculated high risk, consider measuring waist circumference and use this to further inform risk level (eg, risk is increased at ≥ 80 cm and high at ≥ 88 cm for women, and increased at ≥ 94 cm and high at ≥ 102 cm for men). 1,6 Be aware these cutoffs vary according to ethnic backgroup of the individual. More information can be found in the NHMRC Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia.
The absolute risk equation currently used in Australia may underestimate CVD risk in:1
- Adults of Aboriginal and Torres Strait Islander descent
- Adults of South Asian, Maori, Pacific Islander and Middle Eastern descent
- Adults with diabetes
- Adults aged over 74 years
- Adults with socioeconomic disadvantage
- Adults with depression
Use pre-treatment measurements for patients already receiving medication
The Framingham risk equation is designed to calculate risk using measurements obtained before pharmacological treatment.1 Therefore, the aim is to use the most recently recorded pre-treatment measure to estimate risk. Blood test results within 5 years can be used. If pre-treatment values are not available or considered clinically inappropriate, use on-treatment values recognising that they may underestimate risk.
What about elevated blood pressure in young children, teenagers or younger adults (45 years)?
Confirm high BP using repeated valid BP measurements. Investigate to rule out secondary hypertension.7,8
Cardiovascular risk calculators
- Australian Cardiovascular Disease Risk Charts (external link to Heart Foundation of Australia website).
- Online cardiovascular disease risk calculator (external link to www.cvdcheck.org.au).
- Quick reference guide to absolute cardiovascular disease risk assessment (external link to
References
- National Vascular Disease Prevention Alliance. Guidelines for the management of absolute cardiovascular disease risk. 2012.
- Nelson MR. Management of high blood pressure in those without overt cardiovascular disease utilising absolute risk scores. Int J Hypertens 2011;2011:595791.
- Zomer E, Owen A, Magliano DJ, et al. Validation of two Framingham cardiovascular risk prediction algorithms in an Australian population: the 'old' versus the 'new' Framingham equation. Eur J Cardiovasc Prev Rehabil 2011;18:115-20.
- Brindle P, Beswick A, Fahey T, et al. Accuracy and impact of risk assessment in the primary prevention of cardiovascular disease: a systematic review. Heart 2006;92:1752-9.
- Wang Z and Hoy WE. Is the Framingham coronary heart disease absolute risk function applicable to Aboriginal people? Med J Aust 2005;182:66-9.
- National Health and Medical Research Council. Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia. Melbourne: Australian Government, 2013 (accessed 4 December 2014).
- National Heart Foundation of Australia. Guideline for the diagnosis and management of hypertension in adults - 2016. Melbourne: National Heart Foundation of Australia, 2016 (accessed 5 July 2021)).
- Ayer JG and Sholler GF. Cardiovascular risk factors in Australian children: hypertension and lipid abnormalities. Aust Prescr 2012;35:51-5.